Donald Roberdeau
2020-11-26 01:05:30 UTC
Good Day.... FYI .... https://www.medpagetoday.com/emergencymedicine/emergencymedicine/89772?fbclid=IwAR3zOv5CS7u-iZDZ5Qu883luGYHVbWporeW6egcp2X-8pw8Bm_T6ia0t7Tc
<QUOTE>
JFK in Trauma Room One: A Witness Remembers
— At just 25, Joe Goldstrich, MD, was the youngest member of the
Ke= nnedy treatment team
by Randy Dotinga, Contributing Writer, MedPage Today November 18, 2020
( PHOTO Loading Image... )
)
Earlier this month, MedPage Today published an article about a
presentation at the annual conference of the American College of Emergency
Physicians regarding the treatment of President John F. Kennedy in the
emergency room of Parkland Memorial Hospital in Dallas on Nov. 22, 1963 --
57 years ago this month. Retired Iowa cardiologist Joe Goldstrich, MD,
responded in the article's comments, noting that he was "the most junior
person actively participating in the JFK resuscitation efforts."
MedPage Today confirmed that Goldstrich was present in Trauma Room One and
reached out to the physician, who is now an advocate for medical cannabis.
In an interview, Goldstrich – 25 years old then and 82 now --
spoke about treating the president, nearly treating his assassin, and his
one regret.
MedPage Today: What do you remember about Nov. 22, 1963?
Joe Goldstrich, MD: I was a fourth-year medical student on my neurosurgery
rotation at Parkland Hospital. Early that morning, we performed an
anterior cervical discectomy on a patient. It was the first time this
procedure had been done at Parkland. Dr. Kemp Clark, who was the head of
neurosurgery, said the main complication that concerned him for this
procedure was that there might be bleeding and it could obstruct the
airway, and the patient might need a tracheotomy.
He asked me: Do you know how to do a tracheotomy? And I said yes. Well, I
had done one on a cadaver, but I wasn't really an expert. So I spent the
whole morning in the library reading up on tracheotomies, and I checked in
on the patient a couple of times to see if he was doing OK.
Then there was a STAT page for Dr. Clark around 12 noon. I was in the
cafeteria on the first floor of the hospital eating lunch. My first
thought was that the reason they were paging Dr. Clark was that this
patient had bled and now has obstruction of his airway. And I'm gonna have
to do a tracheotomy.
I ran up five or six flights of stairs to the floor where the patient was,
and I burst into the room. He was sitting in bed, reading a magazine. I
said, "Oh, thank God you're OK. You're fine. They're paging Dr. Clark
STAT, and I had no idea what it was and thought it might have been you."
He said, "I don't know," but he pointed out the window to where the
Kennedy motorcade was pulling into the entrance of the hospital. "Maybe it
has something to do with those limousines that are going into the
hospital."
I ran down the stairs to the emergency room. I was in my scrubs from the
morning. There was already a Secret Service agent at the door. I said
"Goldstrich, neurosurgery," and he let me right in. I got into the
emergency room at the same time as JFK was entering on a gurney.
( PHOTO Loading Image...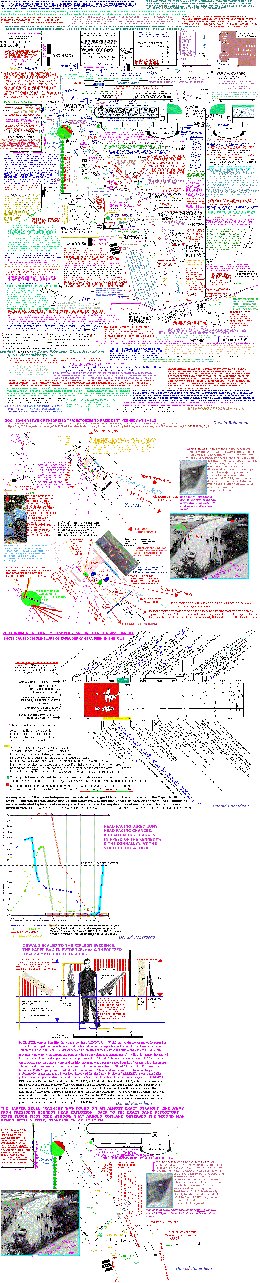 )
)
(PHOTO CAPTION)Retired Iowa cardiologist, Joe Goldstrich, MD
Did you realize the patient was Kennedy?
I knew that it was. I don't remember exactly how, but I knew.
What was your job in Trauma Room One?
I helped move him from the gurney to the treatment table and then undress
him.
I was also the chief gofer. I went to get the defibrillator, which was
about the size of a single-door refrigerator. I pushed it on the casters
back from another part of the emergency room to Trauma Room One.
What struck you about his condition?
I saw the wound in the lower part of his neck. I looked in the neck wound
and saw the cartilage of the trachea on the back side through the hole. I
do not remember whether instruments had [yet] been used to expand the
wound. I am clear, however, that I saw the posterior aspect of the
trachea.
What happened next?
Within a few minutes, there were a number of people in Trauma Room One.
When Dr. Clark walked in, [emergency room director] Dr. Charlie Baxter was
doing closed-chest cardiac compressions on JFK. Dr. Clark saw the head
wound and said something like, "My God, Charlie, what are you doing? His
brains are on the floor."
At that moment I was standing on the left side of Kennedy. And Jackie
[Kennedy] was further back on his right side, in a corner. Dr. Clark had
not seen Jackie. When he did see her, I was right between them. I saw her
expression when she heard what he had said. That's another moment that's
indelibly imprinted on my brain, unfortunately.
What did you see?
Jackie was in shock, like a deer in the headlights. She was surprised that
someone spoke so bluntly about what was going on.
Do you think Kennedy was alive when he reached the hospital?
He was dead on arrival, in all likelihood. I'm not the expert on that.
That's just my humble, amateur opinion.
You didn't talk publicly about assisting in Trauma Room One until you
appeared in the 1993 book JFK: Breaking the Silence. How come?
Because I was afraid. There were so many people who were associated with
the assassination who had died, sometimes by questionable means. Then this
guy [author Bill Sloan] tracked me down and wanted an interview. He called
me a couple of times, and I said no. And then when he called me again, and
I said to myself, "Well, maybe this professional writer can help me with
the book that I was writing [about antioxidants and heart disease]."
I gave him the interview. It turned out he knew nothing about medicine,
and he was no help whatsoever. But that's what drew me out of my shell.
At first, you believed that JFK was shot in the throat from the front, suggesting the possibility of a second shooter. What changed your mind?
When I first saw that wound in Trauma Room One, I did not know anything
about ballistics and entrance and exit wounds. Then I went into the army
in 1965, and I was stationed in the Dominican Republic. After a crash
course in entrance and exit wounds by the field hospital commander, I was
sent to examine the wound of a Dominican who'd been shot by an American
MP. Based on what I had learned, it was clear to me that the Dominican was
shot in the back. In that moment, I realized that JFK's throat wound was
probably an entrance wound because the margins were so clean and the wound
was so small.
But over the past couple of years, I spent a considerable amount of time watching the Zapruder film. After watching it over and over again, I realized it would be impossible for someone from the front to shoot Kennedy simultaneously with [Lee Harvey] Oswald shooting from behind the president. That's when I changed my mind. However, no one will ever know for sure.
Do you think JFK got excellent care?
Absolutely. He got state-of-the-art care. As students, we were told that Parkland had some of the best survival rates in the whole country for trauma patients. This was supposedly due to Dr. Tom Shires, the chief of surgery, popularizing the use of intravenous fluids acutely rather than blood transfusions. The staff and residents in the emergency room were successfully working with trauma patients on a daily basis. At least, that is what I was told as a medical student back then.
Were you a fan of the president?
I loved him. I resonated with his philosophy and his agenda. I guess I was a major JFK fan.
There's something else: One my best friends growing up in Dallas was named Henry Zapruder. His father was Abraham Zapruder [the Dallas dressmaker who shot the famous film of the assassination.] I knew the Zapruders very well, and had been in their home many times. [Editor's note: MedPage Today reached out to the Zapruder family, which confirms the close friendship.]
What did you do after JFK was declared dead?
I went into the surgical dressing room and probably put on my street clothes. Then I went outside. There was a big crowd across the street in front of the nursing school dormitory. I just went and mingled in that crowd. I didn't say a word. I didn't tell anybody that I was there. I just listened to what they said. And then I went home.
It must have been a shock to my immune system. On Saturday [Nov. 23] the next day, I had a bad case of the flu when I woke up. But I was on call on surgery on Sunday [Nov. 24], and I came to the hospital even though I was sick.
A third-year student named Nick Grivas, who went on to become a neurosurgeon, was also on surgery call that day. I told Nick, "I'm gonna go to the call room and get some rest because I'm not feeling well. But if anything happens, come wake me up."
When I woke up from my nap and came out into the surgical area, people were running around. I learned that Oswald had been shot and was being operated on. Nick Grivas had scrubbed in my place.
Do you have any regrets about those moments in Trauma Room One?
Yes. When I looked at JFK's throat wound, my thoughts were that it was not necessary to expand the hole for the tracheotomy. They could have put the tracheotomy tube directly into the hole without the incisions that were done. I wanted to say that when they started to do the tracheotomy: "You don't have to do that."
But remember, I was the most junior person in the room. These were my professors, surgeons and residents who were years ahead of me in their training. So I did not say, "Just put it in the hole, you don't have to do any cutting." That would have preserved the nature of the wound, making it more amenable to determining whether it was an entrance or an exit wound.
But I didn't say anything. I regret that.
Last Updated November 18, 2020
<END QUOTE>
Best Regards in 112263 Research,
Don
Donald Roberdeau
United States Navy
U.S.S. John F. Kennedy, CV-67, plank walker
Sooner, or later, The Truth emerges clearly
For your key considerations + independent determinations....
Homepages Website: "Men of Courage": President Kennedy-elimination
Evidence, Witnesses, Photographers, Outstanding Researchers Discoveries,
Suspects, + Key Considerations....
http://droberdeau.blogspot.com/.../1-men-of-courage-jfk...
The Dealey Plaza Detailed Map: Documented 11-22-63 Victims Precise
Locations + Reactions, Evidence, Witnesses Locations, Photographers,
Suspected Bullet Trajectories, Outstanding Researchers Discoveries, +
Important Information + Key Considerations, in One Convenient Resource....
Loading Image...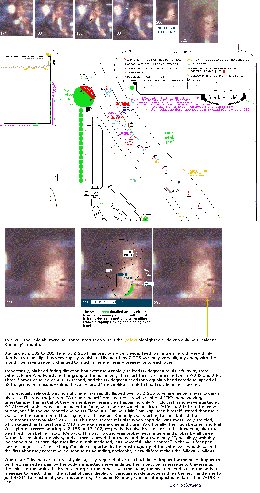
(updated map, + with new information)
Discovery: Very Close JFK Assassination Witness ROSEMARY WILLIS's
Zapruder Film Documented 2nd Head Snap: West, Ultrafast, and Directly
Towards the Grassy Knoll....
http://droberdeau.blogspot.com/.../discovery-close-jfk...
Visual Report: The First Bullet Impact Into President Kennedy: While
JFK was Still Hidden Under the "Magic-limbed-ricochet-tree"....
Loading Image...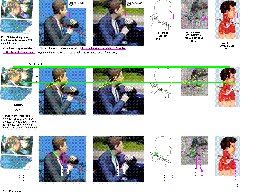
Visual Report: Reality Versus C.A.D.: the Real World, versus,
Garbage-in-garbage-out....
Loading Image...
T ogether
E veryone
A chieves
M ore
Terrorism Alert For the United States:
Loading Image...
http://www.dhs.gov
<QUOTE>
JFK in Trauma Room One: A Witness Remembers
— At just 25, Joe Goldstrich, MD, was the youngest member of the
Ke= nnedy treatment team
by Randy Dotinga, Contributing Writer, MedPage Today November 18, 2020
( PHOTO Loading Image...
 )
)Earlier this month, MedPage Today published an article about a
presentation at the annual conference of the American College of Emergency
Physicians regarding the treatment of President John F. Kennedy in the
emergency room of Parkland Memorial Hospital in Dallas on Nov. 22, 1963 --
57 years ago this month. Retired Iowa cardiologist Joe Goldstrich, MD,
responded in the article's comments, noting that he was "the most junior
person actively participating in the JFK resuscitation efforts."
MedPage Today confirmed that Goldstrich was present in Trauma Room One and
reached out to the physician, who is now an advocate for medical cannabis.
In an interview, Goldstrich – 25 years old then and 82 now --
spoke about treating the president, nearly treating his assassin, and his
one regret.
MedPage Today: What do you remember about Nov. 22, 1963?
Joe Goldstrich, MD: I was a fourth-year medical student on my neurosurgery
rotation at Parkland Hospital. Early that morning, we performed an
anterior cervical discectomy on a patient. It was the first time this
procedure had been done at Parkland. Dr. Kemp Clark, who was the head of
neurosurgery, said the main complication that concerned him for this
procedure was that there might be bleeding and it could obstruct the
airway, and the patient might need a tracheotomy.
He asked me: Do you know how to do a tracheotomy? And I said yes. Well, I
had done one on a cadaver, but I wasn't really an expert. So I spent the
whole morning in the library reading up on tracheotomies, and I checked in
on the patient a couple of times to see if he was doing OK.
Then there was a STAT page for Dr. Clark around 12 noon. I was in the
cafeteria on the first floor of the hospital eating lunch. My first
thought was that the reason they were paging Dr. Clark was that this
patient had bled and now has obstruction of his airway. And I'm gonna have
to do a tracheotomy.
I ran up five or six flights of stairs to the floor where the patient was,
and I burst into the room. He was sitting in bed, reading a magazine. I
said, "Oh, thank God you're OK. You're fine. They're paging Dr. Clark
STAT, and I had no idea what it was and thought it might have been you."
He said, "I don't know," but he pointed out the window to where the
Kennedy motorcade was pulling into the entrance of the hospital. "Maybe it
has something to do with those limousines that are going into the
hospital."
I ran down the stairs to the emergency room. I was in my scrubs from the
morning. There was already a Secret Service agent at the door. I said
"Goldstrich, neurosurgery," and he let me right in. I got into the
emergency room at the same time as JFK was entering on a gurney.
( PHOTO Loading Image...
 )
)(PHOTO CAPTION)Retired Iowa cardiologist, Joe Goldstrich, MD
Did you realize the patient was Kennedy?
I knew that it was. I don't remember exactly how, but I knew.
What was your job in Trauma Room One?
I helped move him from the gurney to the treatment table and then undress
him.
I was also the chief gofer. I went to get the defibrillator, which was
about the size of a single-door refrigerator. I pushed it on the casters
back from another part of the emergency room to Trauma Room One.
What struck you about his condition?
I saw the wound in the lower part of his neck. I looked in the neck wound
and saw the cartilage of the trachea on the back side through the hole. I
do not remember whether instruments had [yet] been used to expand the
wound. I am clear, however, that I saw the posterior aspect of the
trachea.
What happened next?
Within a few minutes, there were a number of people in Trauma Room One.
When Dr. Clark walked in, [emergency room director] Dr. Charlie Baxter was
doing closed-chest cardiac compressions on JFK. Dr. Clark saw the head
wound and said something like, "My God, Charlie, what are you doing? His
brains are on the floor."
At that moment I was standing on the left side of Kennedy. And Jackie
[Kennedy] was further back on his right side, in a corner. Dr. Clark had
not seen Jackie. When he did see her, I was right between them. I saw her
expression when she heard what he had said. That's another moment that's
indelibly imprinted on my brain, unfortunately.
What did you see?
Jackie was in shock, like a deer in the headlights. She was surprised that
someone spoke so bluntly about what was going on.
Do you think Kennedy was alive when he reached the hospital?
He was dead on arrival, in all likelihood. I'm not the expert on that.
That's just my humble, amateur opinion.
You didn't talk publicly about assisting in Trauma Room One until you
appeared in the 1993 book JFK: Breaking the Silence. How come?
Because I was afraid. There were so many people who were associated with
the assassination who had died, sometimes by questionable means. Then this
guy [author Bill Sloan] tracked me down and wanted an interview. He called
me a couple of times, and I said no. And then when he called me again, and
I said to myself, "Well, maybe this professional writer can help me with
the book that I was writing [about antioxidants and heart disease]."
I gave him the interview. It turned out he knew nothing about medicine,
and he was no help whatsoever. But that's what drew me out of my shell.
At first, you believed that JFK was shot in the throat from the front, suggesting the possibility of a second shooter. What changed your mind?
When I first saw that wound in Trauma Room One, I did not know anything
about ballistics and entrance and exit wounds. Then I went into the army
in 1965, and I was stationed in the Dominican Republic. After a crash
course in entrance and exit wounds by the field hospital commander, I was
sent to examine the wound of a Dominican who'd been shot by an American
MP. Based on what I had learned, it was clear to me that the Dominican was
shot in the back. In that moment, I realized that JFK's throat wound was
probably an entrance wound because the margins were so clean and the wound
was so small.
But over the past couple of years, I spent a considerable amount of time watching the Zapruder film. After watching it over and over again, I realized it would be impossible for someone from the front to shoot Kennedy simultaneously with [Lee Harvey] Oswald shooting from behind the president. That's when I changed my mind. However, no one will ever know for sure.
Do you think JFK got excellent care?
Absolutely. He got state-of-the-art care. As students, we were told that Parkland had some of the best survival rates in the whole country for trauma patients. This was supposedly due to Dr. Tom Shires, the chief of surgery, popularizing the use of intravenous fluids acutely rather than blood transfusions. The staff and residents in the emergency room were successfully working with trauma patients on a daily basis. At least, that is what I was told as a medical student back then.
Were you a fan of the president?
I loved him. I resonated with his philosophy and his agenda. I guess I was a major JFK fan.
There's something else: One my best friends growing up in Dallas was named Henry Zapruder. His father was Abraham Zapruder [the Dallas dressmaker who shot the famous film of the assassination.] I knew the Zapruders very well, and had been in their home many times. [Editor's note: MedPage Today reached out to the Zapruder family, which confirms the close friendship.]
What did you do after JFK was declared dead?
I went into the surgical dressing room and probably put on my street clothes. Then I went outside. There was a big crowd across the street in front of the nursing school dormitory. I just went and mingled in that crowd. I didn't say a word. I didn't tell anybody that I was there. I just listened to what they said. And then I went home.
It must have been a shock to my immune system. On Saturday [Nov. 23] the next day, I had a bad case of the flu when I woke up. But I was on call on surgery on Sunday [Nov. 24], and I came to the hospital even though I was sick.
A third-year student named Nick Grivas, who went on to become a neurosurgeon, was also on surgery call that day. I told Nick, "I'm gonna go to the call room and get some rest because I'm not feeling well. But if anything happens, come wake me up."
When I woke up from my nap and came out into the surgical area, people were running around. I learned that Oswald had been shot and was being operated on. Nick Grivas had scrubbed in my place.
Do you have any regrets about those moments in Trauma Room One?
Yes. When I looked at JFK's throat wound, my thoughts were that it was not necessary to expand the hole for the tracheotomy. They could have put the tracheotomy tube directly into the hole without the incisions that were done. I wanted to say that when they started to do the tracheotomy: "You don't have to do that."
But remember, I was the most junior person in the room. These were my professors, surgeons and residents who were years ahead of me in their training. So I did not say, "Just put it in the hole, you don't have to do any cutting." That would have preserved the nature of the wound, making it more amenable to determining whether it was an entrance or an exit wound.
But I didn't say anything. I regret that.
Last Updated November 18, 2020
<END QUOTE>
Best Regards in 112263 Research,
Don
Donald Roberdeau
United States Navy
U.S.S. John F. Kennedy, CV-67, plank walker
Sooner, or later, The Truth emerges clearly
For your key considerations + independent determinations....
Homepages Website: "Men of Courage": President Kennedy-elimination
Evidence, Witnesses, Photographers, Outstanding Researchers Discoveries,
Suspects, + Key Considerations....
http://droberdeau.blogspot.com/.../1-men-of-courage-jfk...
The Dealey Plaza Detailed Map: Documented 11-22-63 Victims Precise
Locations + Reactions, Evidence, Witnesses Locations, Photographers,
Suspected Bullet Trajectories, Outstanding Researchers Discoveries, +
Important Information + Key Considerations, in One Convenient Resource....
Loading Image...

(updated map, + with new information)
Discovery: Very Close JFK Assassination Witness ROSEMARY WILLIS's
Zapruder Film Documented 2nd Head Snap: West, Ultrafast, and Directly
Towards the Grassy Knoll....
http://droberdeau.blogspot.com/.../discovery-close-jfk...
Visual Report: The First Bullet Impact Into President Kennedy: While
JFK was Still Hidden Under the "Magic-limbed-ricochet-tree"....
Loading Image...

Visual Report: Reality Versus C.A.D.: the Real World, versus,
Garbage-in-garbage-out....
Loading Image...

T ogether
E veryone
A chieves
M ore
Terrorism Alert For the United States:
Loading Image...

http://www.dhs.gov


